TEMPEROMANDIBULAR DISORDERS
Orofacial pain, as described by the American Academy of Orofacial Pain, “includes pain disorders associated with hard and soft tissues of the head, face, neck, and all intraoral structures”.
Temporomandibular disorders “include conditions involving the muscles of mastication and/or the temporomandibular joints” (they are the joints which allow the movements of the mandible and are located just in front of the ear) and have been identified as an important cause of non-dental pain in the orofacial region.
The causes of such disorders are various including systemic diseases (rheumatoid arthritis, lupus erithematosus, Lyme disease, tumors, fibromyalgia), traumas, vicious habits (bad posture, tooth grinding and clenching), psychologic factors (stress, depression, anxiety) and an altered dental occlusion. Many of these factors are present in the life of all of us, but our organism can usually adapt until such capacity of adaptation is overcome and the symptoms appear. In fact, in most of the cases, more than one factor is involved in the development of the disorder. For example, it is not unusual for any person to have an imperfect dental occlusion, or to keep an incorrect posture while working on a computer: with the back bent and the head moved forward. As we already mentioned, our organism can usually adapt, but sometimes because of a period of major distress, or because of a trauma, for example a car accident, symptoms can easily appear. Then the most effective treatment is aimed at correcting all the factors which contributed to initiate the problem.
But what are the main symptoms of such disorders?
Symptoms of temporomandibular disorders and the reasons for their occurrence are listed below
Symptoms of temporomandibular disorders are various and non-specific. Non-specific means that they are symptoms also common to other diseases, therefore it is very important a correct “differential diagnosis”, that is the ability to identify what disorder is causing the symptoms among all the possible ones.
The following is a list of symptoms often present in patients with temporomandibular disorders, some are very common, others are less common:
- Jaw joint (TMJ) pain or noises (clicking, popping, or grating)
- Limited mouth opening
- Deviations of mouth opening
- Headache
- Face muscles pain and fatigue
- Neck, shoulders, and back pain and stiffness
- Backache
- Earache
- Ear sounds (tinnitus)
- Ear stuffiness
- Hearing loss
- Pain in the eye or around the eye
- Difficulty focusing
- Dizziness, vertigo
- Arm and hand tingling or numbness
- Toothache
|
|
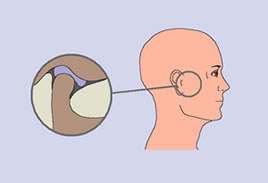

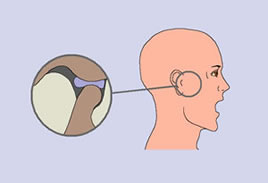
During mouth opening the condyle turns and then slides forward and downwards following the profile of the articular eminence (which is the tubercle in front of the articular cavity), and the articular disc slides forward and downword following the movement of the condyle. During mouth closing the opposite occurs, the condyle slides backward and turns in the opposite way, with the articular disc following the movement of the condyle sliding backward and upward (see figure). When the joint is perfectly healthy the movements of mouth opening and closing occur without any pain, without any joint noise, without deviations of the mandible, and there is no limitation of mouth opening. Also the anterior and lateral movements of the mandible occur without any pain, without any joint noise, and are symmetrical.
Jaw joint (TMJ) pain can have different causes. It is frequently due to an inflammation of the joint, and the cause can be an acute trauma to the mandible, for example because of a fist, or a fall, or because of a car accident; or a trauma of minor intensity, but longer duration related to bruxism, an incorrect dental occlusion or displacement of the articular disc.
Jaw joint (TMJ) pain can have different causes. It is frequently due to an inflammation of the joint, and the cause can be an acute trauma to the mandible, for example because of a fist, or a fall, or because of a car accident; or a trauma of minor intensity, but longer duration related to bruxism, an incorrect dental occlusion or displacement of the articular disc.
Bruxism is the habit of clenching or grinding of the teeth. Such activity generally takes place during sleep, often involuntarily, and commonly during periods of high stress and tension. It can excessively load the TMJs and cause inflammation.
An incorrect dental occlusion, can cause inflammation when forces the mandible to have a position that is not physiological. In fact, the position of the mandible depends on the position of the teeth: we can close the mouth only in the way the teeth “match”.
Sometimes this position is different from the correct position, in such cases the mandible can be placed too forward, backward, or moved laterally. If, for example, the mandible is placed backward, loading of the TMJs is more likely to occur, therefore inflammation can take place. This possibility is more probable if bruxism is present in addition to the incorrect dental occlusion.
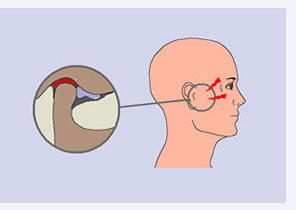
In some cases the articular disc is displaced, that means moved from its position, generally forward and to the side. In such condition, the tissues that are behind the disc are loaded, and since they are rich with blood vessels and nerves, can easily become inflamed (see figure on the side).
Pain coming from inflammation of the TMJ usually worsens while chewing and during mandibular movements, especially opening the mouth fully (for example while yawning, or biting a sandwich).
An incorrect dental occlusion, can cause inflammation when forces the mandible to have a position that is not physiological. In fact, the position of the mandible depends on the position of the teeth: we can close the mouth only in the way the teeth “match”.
Sometimes this position is different from the correct position, in such cases the mandible can be placed too forward, backward, or moved laterally. If, for example, the mandible is placed backward, loading of the TMJs is more likely to occur, therefore inflammation can take place. This possibility is more probable if bruxism is present in addition to the incorrect dental occlusion.
In some cases the articular disc is displaced, that means moved from its position, generally forward and to the side. In such condition, the tissues that are behind the disc are loaded, and since they are rich with blood vessels and nerves, can easily become inflamed (see figure on the side).
Pain coming from inflammation of the TMJ usually worsens while chewing and during mandibular movements, especially opening the mouth fully (for example while yawning, or biting a sandwich).
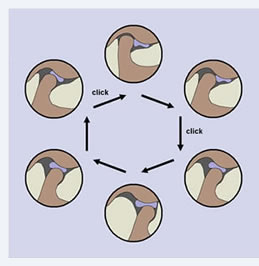
Jaw joint (TMJ) noises during mandibular movements are an indication of the fact that articular movements are not smooth. When the noise heard is a snapping sound like a “click” or “pop”, this is probably due to a displacement of the articular disc. Such displacement occurs when the mouth is closed, but during opening it goes back to the correct position, and this happens with a quick movement that creates the “click”. The opposite happens during mouth closing, when the disc displaces forward again, and generally another “click” can be heard (see figure on the side).
Grating noises (like sand in the joint) are due to degeneration of the articular cartilage which is not completely smooth any more, but rough and irregular. Therefore during mandibular movements rubbing of the articular surfaces creates noises.
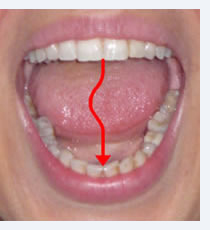
Limitation and deviation of mouth opening are caused by displacement of the articular disc. When such displacement only occurs with the mouth closed and the disc goes back to the correct position during mouth opening, a lateral deviation of the mandible takes place (to the same side of the “click”) during mouth opening, but withfull opening the mandible goes back to the center, and mouth opening is not limited (see figure on the left). But when disc is permanently displaced and does not go back to the correct position, there is an evident lateral deviation of the mandible associated with a limited mouth opening. In this case the “click” is not present any more, and the jaw feels “locked” (figure on the right).
In the first case, when the “click” is present, often the joint does not hurt, while in the second case a severe inflammation of the joint is frequently associated that makes the area very painful. The first condition can change into the second, at first the disc can be able to go back into the correct position during mouth opening, but later the displacement can become permanent and the mandible can become “locked”. Patients often say that for a long time they had clicking noises during mouth opening or while chewing, and suddenly the “click” disappeared, but they could not open the mouth fully.
Grating noises (like sand in the joint) are due to degeneration of the articular cartilage which is not completely smooth any more, but rough and irregular. Therefore during mandibular movements rubbing of the articular surfaces creates noises.
Limitation and deviation of mouth opening are caused by displacement of the articular disc. When such displacement only occurs with the mouth closed and the disc goes back to the correct position during mouth opening, a lateral deviation of the mandible takes place (to the same side of the “click”) during mouth opening, but withfull opening the mandible goes back to the center, and mouth opening is not limited (see figure on the left). But when disc is permanently displaced and does not go back to the correct position, there is an evident lateral deviation of the mandible associated with a limited mouth opening. In this case the “click” is not present any more, and the jaw feels “locked” (figure on the right).
In the first case, when the “click” is present, often the joint does not hurt, while in the second case a severe inflammation of the joint is frequently associated that makes the area very painful. The first condition can change into the second, at first the disc can be able to go back into the correct position during mouth opening, but later the displacement can become permanent and the mandible can become “locked”. Patients often say that for a long time they had clicking noises during mouth opening or while chewing, and suddenly the “click” disappeared, but they could not open the mouth fully.
|

|
Headache is one of the most frequent symptoms. It is commonly due to fatigue to the muscles of mastication, or to the muscles of the head, neck and shoulders, which create pain that spreads involving several areas of the head. Since the muscles involved are generally various, headache can extend to large areas of the head: the temples, the side of the face, the forehead, the back and the top of the head. If such fatigue is caused by night-time bruxism, headache occurs mostly or only on waking up in the morning. Another cause of headache can be pain irradiating from the TMJ. When this joint is inflamed pain is usually located in front of the ear, but when it is more intense, for example during chewing, it can irradiate to the surrounding areas, especially to the temple and the side of the head. Sometimes these episodes of headache can be confused with migraine attacks, because they can show up in the same way.
Face muscles pain and fatigue is related to fatigue to the muscles due to bruxism sometimes associated with dental malocclusion. Depending on which muscles are involved pain can be felt in different areas of the face: mandible and cheeks, the zygomas, temples, teeth, ears. Pain is usually worsened by chewing and mandibular movements.
Patients suffering from temporomandibular disorders frequently also suffer from pain and stiffness to the neck, shoulders and back, of muscular origin. They are caused by the close relationship between dental occlusion, muscular activity, and posture. The muscles affected are tender to palpation and can give pain localized in the muscle, or also referred to different areas of the shoulders, head and neck.
A great percentage of patients report symptoms to the ears going from earache, to ear sounds (tinnitus), to hearing loss and to ear stuffiness. In most of the cases earache is an inflammation of the TMJ that patients refer as “earache” because the joint is very close to the ear, but there is nothing wrong with the ear (as it can be evaluated by an otolaryngologist). Ear sounds, like also earstuffiness and hearing loss, seem to be due to the relationship between the structures of the masticatory system and the inner ear. Mandibular movements and bruxism can affect ear function through muscular, nervous, and ligamentous connections.
Patients suffering from temporomandibular disorders frequently also suffer from pain and stiffness to the neck, shoulders and back, of muscular origin. They are caused by the close relationship between dental occlusion, muscular activity, and posture. The muscles affected are tender to palpation and can give pain localized in the muscle, or also referred to different areas of the shoulders, head and neck.
A great percentage of patients report symptoms to the ears going from earache, to ear sounds (tinnitus), to hearing loss and to ear stuffiness. In most of the cases earache is an inflammation of the TMJ that patients refer as “earache” because the joint is very close to the ear, but there is nothing wrong with the ear (as it can be evaluated by an otolaryngologist). Ear sounds, like also earstuffiness and hearing loss, seem to be due to the relationship between the structures of the masticatory system and the inner ear. Mandibular movements and bruxism can affect ear function through muscular, nervous, and ligamentous connections.

|

|
Eye symptoms involve pain in the eye or around the eye, and difficulty focusing.Pain is usually a referred pain due to suffering of the muscles of the neck, or the cervical spine; other times referred pain can originate from the greater or lesser occipital nerves (they are nerves that come from the neck and innervate the head), that can be irritated because of inflammation, or compression by the muscles of the neck.
Difficulty focusing seems to be related to alteration to the convergence of the eyes caused by dental occlusion. Patients suffering from temporomandibular disorders have higher prevalence of defects of convergence, especially associated with headache, neck and shoulder pain, masticatory muscles pain, and limited mouth opening.
Dizziness, and sometimes also vertigo, are due to spasm and fatigue to the muscles of the neck and shoulders, in fact they are similar to the symptoms of the disorders of the cervical spine. As we already mentioned, a close relationship exists between dental occlusion, muscular activity, and posture, and this can cause suffering to different areas of the spine.
Arm and hand tingling or numbness occurwhen the nerves going to the arms and hands are compressed where they origin at the base of the neck. Either by the neck muscles, when they are contracted and fatigued, or because of changes to the posture of the cervical spine.
Toothache can be caused by compression of the teeth in case of bruxism. Tooth grinding and clenching creates a serious loading to the teeth, that can become tender or sensitive. it is frequent that bruxism be mostly nocturnal, in this case pain is typically felt in the morning on waking up. In other cases toothache can be of muscular origin but referred to the teeth. The muscles that can be responsible are the muscles of mastication corresponding to the cheeks and temples, that are usually tender.
Obviously, any toothache caused by local factors like decay (cavities) or gingival inflammation, or other lesions of the mouth must be ruled out.
Difficulty focusing seems to be related to alteration to the convergence of the eyes caused by dental occlusion. Patients suffering from temporomandibular disorders have higher prevalence of defects of convergence, especially associated with headache, neck and shoulder pain, masticatory muscles pain, and limited mouth opening.
Dizziness, and sometimes also vertigo, are due to spasm and fatigue to the muscles of the neck and shoulders, in fact they are similar to the symptoms of the disorders of the cervical spine. As we already mentioned, a close relationship exists between dental occlusion, muscular activity, and posture, and this can cause suffering to different areas of the spine.
Arm and hand tingling or numbness occurwhen the nerves going to the arms and hands are compressed where they origin at the base of the neck. Either by the neck muscles, when they are contracted and fatigued, or because of changes to the posture of the cervical spine.
Toothache can be caused by compression of the teeth in case of bruxism. Tooth grinding and clenching creates a serious loading to the teeth, that can become tender or sensitive. it is frequent that bruxism be mostly nocturnal, in this case pain is typically felt in the morning on waking up. In other cases toothache can be of muscular origin but referred to the teeth. The muscles that can be responsible are the muscles of mastication corresponding to the cheeks and temples, that are usually tender.
Obviously, any toothache caused by local factors like decay (cavities) or gingival inflammation, or other lesions of the mouth must be ruled out.
|

|
Management of temporomandibular disorders is achieved by a multidisciplinary approach, which includes interventions intended to improve the health of the different compartments of the organism that can be involved This means that competence of different specialists in different fields of medicine can be necessary.
The dentist can work by correcting dental occlusion. This can be achieved by the use of resin removable transparent appliances (also called splints, night-guards, orthotics), that cover the surface of the teeth, upper or lower, and allow to change the way they come in contact, modifying dental occlusion, and consequently temporarily correcting the position of the mandible (see figures). In most of the cases no definitive treatment is needed, but in some selected cases a permanent change of dental occlusion, maintaining the position achieved by the use of the dental appliance, can be indicated. Such interventions need to be evaluated case by case, however, the alternatives are: an orthodontic treatment (the so-called “braces”), or a prosthetic treatment (crowns or bridges), or, in the simplest cases, the surfaces of the teeth can be adjusted by the use of materials for dental restorations or removing minor interferences. Dental appliances are also very useful to limit damage and reduce the symptoms caused by bruxism.
When the cause that precipitated or contributed to the symptoms is not limited to an altered dental occlusion, or bruxism, but other variables are involved, the dentist needs to be helped by other specialists. Physiatrists, chiropractors, physical therapists, osteopaths are important for the management of patients who complain about pain or stiffness in the neck, shoulders, back, and who need specific interventions to sites different from the mouth.
Neurologists are important for the evaluation of patients with headache not related to dental occlusion and bruxism, or patients with real nerve lesions both to the peripheral and central nervous system.
Psychologists and psychiatrists are important when psychologic factors (stress, anxiety, depression, somatization) are involved in the perpetuation of the symptoms.
Positive results have also been achieved with acupuncture, acupressure, meditation and hypnosis.
The dentist can work by correcting dental occlusion. This can be achieved by the use of resin removable transparent appliances (also called splints, night-guards, orthotics), that cover the surface of the teeth, upper or lower, and allow to change the way they come in contact, modifying dental occlusion, and consequently temporarily correcting the position of the mandible (see figures). In most of the cases no definitive treatment is needed, but in some selected cases a permanent change of dental occlusion, maintaining the position achieved by the use of the dental appliance, can be indicated. Such interventions need to be evaluated case by case, however, the alternatives are: an orthodontic treatment (the so-called “braces”), or a prosthetic treatment (crowns or bridges), or, in the simplest cases, the surfaces of the teeth can be adjusted by the use of materials for dental restorations or removing minor interferences. Dental appliances are also very useful to limit damage and reduce the symptoms caused by bruxism.
When the cause that precipitated or contributed to the symptoms is not limited to an altered dental occlusion, or bruxism, but other variables are involved, the dentist needs to be helped by other specialists. Physiatrists, chiropractors, physical therapists, osteopaths are important for the management of patients who complain about pain or stiffness in the neck, shoulders, back, and who need specific interventions to sites different from the mouth.
Neurologists are important for the evaluation of patients with headache not related to dental occlusion and bruxism, or patients with real nerve lesions both to the peripheral and central nervous system.
Psychologists and psychiatrists are important when psychologic factors (stress, anxiety, depression, somatization) are involved in the perpetuation of the symptoms.
Positive results have also been achieved with acupuncture, acupressure, meditation and hypnosis.

|

|
